









空鼻症-邱昱勳醫師的台灣病患經驗分享-Empty Nose Syndrome -The Taiwanese Experience with Dr. Tony Chiu - S4 - EP03
分類:整形學術研討

邱昱勳醫師指出,空鼻症是1994年才被醫生提出來的病症,有很多醫生並不了解這種病;由於近年個案有越來越多的趨勢,才逐漸備受重視。其發生的原因可能為感染或進行鼻甲雷射手術、鼻中膈手術時,切除太多鼻甲,使鼻腔空間變大及鼻黏膜、鼻腔神經遭到破壞,導致患者吸入空氣時,吸入鼻腔的空氣變成「渦流」或「亂流」。
手術方面又分為傳統的縫合鼻孔、鼻竇內視鏡進行微創手術等兩種方式;傳統方法是縫合鼻孔,但會造成外觀及生活上的不便;而鼻竇內視鏡進行微創手術,使用材料可為人工合成物或自體組織移植,依病人本身條件及需求而異,不同材料各有其優缺點。
而近年國外論文研究發現,自體軟骨移植為更好的方法,術後感染及排斥的風險低。因此,邱昱勳醫師在和患者黃女士充分溝通後,採用患者本身耳軟骨進行下鼻甲新生手術,重建ㄧ個新的下鼻甲,術後傷口恢復良好,至今2個多月不但鼻塞不再復發,整個人也開朗多了,患者非常滿意手術結果,此為國內首例自體軟骨下鼻甲新生術。

<蘋果新聞>隆鼻30年婦眼腫如被家暴
一名60歲婦人,30多年前手術隆鼻,近一年多來,隆鼻處山根反覆紅腫,有時更是腫到雙眼張不開,像個被家暴的婦女,但卻不會痛,醫師認為是身體對隆鼻物產生排斥反應,經手術清出隆鼻物,婦人才告別動輒腫眼日子。醫師指,若婦人再不取出隆鼻物,有可能會因腫脹壓迫視神經,有失明危險。
【榮登國際權威】邱昱勳醫師學術成果發表於《PRS Global Open》
邱昱勳醫師長期致力於鼻整形研究,其針對「空鼻症(Empty Nose Syndrome)」的創新治療研究,於 2026 年正式發表於美國整形外科醫師協會(ASPS)官方學術期刊,象徵台灣醫療技術接軌國際。
RECONSTRUCTIVE: CASE REPORT
Empty Nose Syndrome Treated With Inferior Turbinate Augmentation Using Homologous Costal Cartilage
Chiu, Yu-Hsun MD, PhD*; Hao, Chung-Yu MD*; Kuo, Yu-Xiang MD*; Hung, Wei-Li MBBS†
Author Information
Plastic & Reconstructive Surgery-Global Open 14(2):p e7466, February 2026. | DOI: 10.1097/GOX.0000000000007466
Summary:
Empty nose syndrome (ENS) is a debilitating, iatrogenic condition caused by a previous inferior turbinectomy; the symptoms of which include subjective feelings of suffocation despite an objectively patent nasal passage. The definitive treatment for ENS is to replace the missing tissue through surgery. The implantation material and the implantation site are important considerations when it comes to ENS surgery. Here, we present a case of ENS treated with inferior turbinate augmentation using homologous costal cartilage. This novel surgical technique creates a submucosal pocket at the site of the inferior turbinate remnant and implants the homologous costal cartilage therein, thus augmenting the inferior turbinate remnant instead of creating a new turbinate. Our case reported a favorable outcome with no obvious complications. This is a rare case report of an ENS treated with inferior turbinate augmentation by using homologous costal cartilage and offers more insight into ENS surgery.
Empty nose syndrome (ENS) was first introduced in 1994 by Eugene Kern and Monika Stenkvist, who recognized it as a complication of turbinate surgery.1 It is an iatrogenic disorder defined by the presence of paradoxical nasal obstruction despite an objectively wide, patent nasal passage caused by previous inferior turbinectomy. Symptoms may include feelings of suffocation, nasal dryness, a burning sensation or pain in the nose, and nasal obstruction. Diagnosis is clinical but can be supported by results from the cotton test, the Empty Nose Syndrome 6-item Questionnaire (ENS6Q), and computed tomography imaging.1 The definitive treatment is to replace the missing tissue through surgery.
Important considerations in terms of ENS surgery include the implantation material and the implantation site. To date, multiple implantation materials have been used, and most implants are placed either on the inferior or lateral nasal wall to form a new turbinate.1,2 In the case featured here, we used a homologous costal cartilage due to its low infection rates and high biocompatibility.3 Furthermore, instead of implanting the homologous costal cartilage on the inferior or lateral nasal wall, we created a submucosal pocket at the site of the inferior turbinate and implanted the homologous costal cartilage therein. This surgical technique helps “augment” the inferior turbinate remnant instead of creating a new turbinate, and may be more physiological.
CASE REPORT
A 39-year-old man presented to our otolaryngology department with complaints of suffocation and a dry nose. According to the patient, he had undergone septomeatoplasty 19 years ago to address nasal obstruction and rhinorrhea. Since then, he had been experiencing feelings of suffocation and a dry nose, which were not relieved by conservative management, such as nasal corticosteroid sprays or oral antihistamines.
On examination, the cotton test was positive. Endoscopic findings revealed a wide-open left nasal passage with limited inferior turbinate volume (Fig. 1A). Computed tomography confirmed a severe reduction in the volume of the left inferior turbinate (Fig. 1B). The patient also scored 18 points on the self-reported ENS6Q and was subsequently diagnosed with ENS. (See table, Supplemental Digital Content 1, which displays preoperative and postoperative ENS6Q scores at 12 mo, https://links.lww.com/PRSGO/E648.)
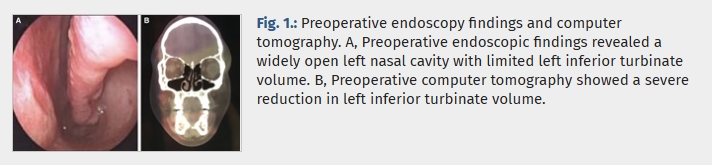
Preoperative endoscopy findings and computer tomography. A, Preoperative endoscopic findings revealed a widely open left nasal cavity with limited left inferior turbinate volume. B, Preoperative computer tomography showed a severe reduction in left inferior turbinate volume.
Here, we introduced an innovative surgical technique involving the creation of a submucosal tunnel at the left inferior turbinate. First, cotton wools were placed anteromedially to the left resected inferior turbinate to estimate the volume required to achieve a good clinical response preoperatively. Second, under endoscopic guidance, local anesthetic was injected submucosally at the site of the left resected inferior turbinate for hydrodissection; this created a plane for our graft to be implanted and reduced the risk of perforation. Third, we dissected along the anterior portion of the remnant concha bone to create a submucosal pocket; the incision was done anteriorly, as there was more mucosa attached to the adjacent lateral wall of the nasal cavity, which could be further dissected if needed, and it allowed better surgical access. (See figure, Supplemental Digital Content 2, which displays the anterior portion of the remnant concha bone that was dissected to create a submucosal pocket. A homologous costal cartilage, carved into a fitting 3-dimensional shape according to the shape and volume of the cotton wools used, was implanted into the submucosal pocket medial to the remnant turbinate bone under endoscopic assistance, https://links.lww.com/PRSGO/E649.) If perforation were to occur, either fascia would be placed underneath the mucosa or a suture would be used to repair the perforation. Fourth, a homologous costal cartilage, carved into a fitting 3-dimensional shape according to the shape and volume of cotton wools used, was implanted into the submucosal pocket medial to the remnant turbinate bone under endoscopic assistance; medial position allowed sturdier positioning and was closer to the nasal valve, which maximized nasal resistance (Supplemental Digital Content 2, https://links.lww.com/PRSGO/E649). The homologous costal cartilage was placed such that the rounded cortical portion faced the medial border of the inferior turbinate remnant, whereas the straight cancellous portion faced the lateral wall of the nasal cavity. Finally, the incision site was sutured with a 5-0 chromic suture.
Postoperative endoscopic findings at 6 months revealed a significant increase in the volume of the left inferior turbinate (Fig. 2A). This positive outcome was further supported by the postoperative computed tomography at 6 months (Fig. 2B). The patient’s ENS6Q score, assessed 12 months after the operation, improved to 8, indicating a notable improvement compared with the preoperative score (Supplemental Digital Content 1, https://links.lww.com/PRSGO/E648).
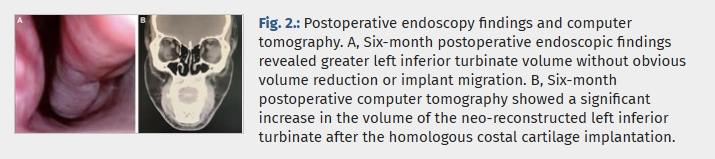
Postoperative endoscopy findings and computer tomography. A, Six-month postoperative endoscopic findings revealed greater left inferior turbinate volume without obvious volume reduction or implant migration. B, Six-month postoperative computer tomography showed a significant increase in the volume of the neo-reconstructed left inferior turbinate after the homologous costal cartilage implantation.
DISCUSSION
When it comes to the management of ENS, conservative options include intranasal irrigation, topical ointment, antibiotic sprays, aerosols, and local corticosteroids.4 However, when conservative therapy proves to be ineffective, surgical management is recommended. Surgical management for ENS includes both injections and implants.
Injections such as hyaluronic acid, platelet-rich plasma, and lipoaspirates have been used, but their effectiveness tends to decrease after 3–6 months.5 In contrast, the effects of implants tend to be longer-lasting, and the choice of implant materials and implantation sites is an important consideration that may impact the outcome.1,2 Numerous implant materials have been used, such as autologous dermal fat and cartilages (septal, conchal, costal); homologous costal cartilage; acellular dermis graft; xenografts, such as porcine small intestine; and synthetic materials, such as polyethylene implants, silastic sheets, and beta-tricalcium phosphate implants, all of which have been shown to improve clinical outcomes.5 However, each of them has its own shortcomings. Harvesting autologous tissue creates an additional wound, which may increase postoperative pain, and site-specific complications include pneumothorax in the case of costal cartilage and limited material in the case of auricular cartilage.6 Similarly, synthetic materials have higher migration and infection rates.1 In our case, we prefer using homologous costal cartilage, which has been used previously by Malik et al7 and Chang et al8 to augment the inferior meatus in ENS surgery, with improved clinical outcomes. We prefer this material because it has advantages such as lower infection rates and higher biocompatibility when compared with synthetic implants.1,3,9 Furthermore, there was no difference in outcomes between autologous and homologous costal cartilage grafts in terms of rates of warping, resorption, infection, contour irregularity, or revision surgery when used in rhinoplasty.3
Our surgical implantation site is unconventional. Standard implantation sites include the lateral nasal wall of the inferior meatus or the inferior wall of the nasal cavity.2 A previous study has shown that lateral nasal wall implantation had better outcomes when compared with inferior wall implantation in terms of the rhinological symptoms, and it was hypothesized to be due to its more realistic representation of the missing inferior turbinate.2 In our case, we created a submucosal pocket at the site of the inferior turbinate and implanted the homologous costal cartilage therein, thus recreating the original resected inferior turbinate through augmentation. This is different from inferior meatus augmentation, where the incision is made more anteriorly at the limen nasi, and a neoturbinate is formed more inferiorly at the inferior meatus.7,8 Inferior turbinate augmentation is more physiological and has achieved favorable outcomes. However, it is surgically more demanding and requires the presence of an inferior turbinate remnant. This is a rare case report of an ENS treated with inferior turbinate augmentation using homologous costal cartilage and offers further insight into ENS surgery.
DISCLOSURE
The authors have no financial interest to declare in relation to the content of this article.
PATIENT CONSENT
Written informed consent was obtained from the legally authorized representative(s) for the anonymized patient information to be published in this article.
ACKNOWLEDGMENTS
Ethical approval to report this case was obtained from the institutional review board of Shin Kong Wu Ho-Su Memorial Hospital (approval ID: 20230501R). All procedures in this study were conducted in accordance with the institutional review board.
REFERENCES
1. Talmadge J, Nayak JV, Yao W, et al. Management of postsurgical empty nose syndrome. Facial Plast Surg Clin North Am. 2019;27:465–475.
• Cited Here |
• Google Scholar
2. Lee TJ, Fu CH, Wu CL, et al. Surgical outcome for empty nose syndrome: Impact of implantation site. Laryngoscope. 2018;128:554–559.
• Cited Here |
• Google Scholar
3. Vila PM, Jeanpierre LM, Rizzi CJ, et al. Comparison of autologous vs homologous costal cartilage grafts in dorsal augmentation rhinoplasty. JAMA Otolaryngol Head Neck Surg. 2020;146:347–354.
• Cited Here |
• Google Scholar
4. Saafan ME, Hegazy HM, Albirmawy OA. Empty nose syndrome: etiopathogenesis and management. Egypt J Otolaryngol. 2016;32:119–129.
• Cited Here |
• Google Scholar
5. Kim DH, Basurrah MA, Kim SW, et al. Surgical and regenerative treatment options for empty nose syndrome: a systematic review. Clin Exp Otorhinolaryngol. 2024;17:241–252.
• Cited Here |
• Google Scholar
6. Hosokawa Y, Miyawaki T, Omura K, et al. Surgical treatment for empty nose syndrome using autologous dermal fat: evaluation of symptomatic improvement. Ear Nose Throat J. 2022;104:1455613221130885.
• Cited Here |
• Google Scholar
7. Malik J, Dholakia S, Spector BM, et al. Inferior meatus augmentation procedure (IMAP) normalizes nasal airflow patterns in empty nose syndrome patients via computational fluid dynamics (CFD) modeling. Int Forum Allergy Rhinol. 2021;11:902–909.
• Cited Here |
• Google Scholar
8. Chang MT, Bartho M, Kim D, et al. Inferior meatus augmentation procedure (IMAP) for treatment of empty nose syndrome. Laryngoscope. 2022;132:1285–1288.
• Cited Here |
• Google Scholar
9. Hu HC, Fang HW, Chiu YH. Delayed-onset edematous foreign body granulomas 40 years after augmentation rhinoplasty by silicone implant combined with liquid silicone injection. Aesthetic Plast Surg. 2017;41:637–640.
• Cited Here |
• Google Scholar





![]()
![]()
